Selon la plupart des manuels de biologie, le principal principe d'organisation de la cellule est la membrane. Les bicouches lipidiques enveloppent les organites, y compris le noyau, les mitochondries et le réticulum endoplasmique, pour garder certaines protéines à l'intérieur et d'autres à l'extérieur.
Le reste de la machinerie interne d'une cellule est décrit comme flottant dans le cytoplasme, avec des protéines qui se heurtent parfois à des partenaires de liaison, des substrats et des médicaments à petites molécules.
De nombreux scientifiques ont soudainement réalisé que leurs protéines préférées subissaient des transitions de phase biologiquement pertinentes et ils ne l'avaient même pas réalisé.
Les condensats biomoléculaires sont des agrégats de molécules sans membrane, telles que les protéines et les acides nucléiques, qui s'organisent dynamiquement pour exécuter un large éventail de fonctions cellulaires.
Il y a une appréciation croissante de l'importance des condensats biomoléculaires et cela oblige les biologistes cellulaires à repenser le modèle classique de la cellule.
Il y a de nombreux exemples d'agrégats moléculaires. Par exemple les granules de glycogène dans les cellules hépatiques et musculaires, les gouttelettes lipidiques dans les cellules graisseuses, les granules pigmentaires dans certaines cellules de la peau et des cheveux et les cristaux de divers types. Ces structures ont été observées pour la première fois par O. F. Müller en 1786.
Les recherches menées au cours de la dernière décennie, ont montré que les perturbations du comportement des condensats jouent un rôle causal dans une myriade de maladies humaines.
Dans la sclérose latérale amyotrophique (SLA) et la dystrophie myotonique de type 1, un corpus solide de littérature indique un rôle causal de la dérégulation des condensats biomoléculaires.
Dès le début, il semblait possible que ces gouttelettes transitoires puissent servir de récipients de réaction cellulaires: accélérer les réactions en concentrant les réactifs ou les ralentir en séparant les réactifs. Plus récemment, les chercheurs ont démêlé leur rôle biologique à la fois dans la santé et dans la maladie.
En 2012, Michael Rosen, a exploré les propriétés biophysiques des condensats biomoléculaires.
L'association avec la maladie a commencé à se cristalliser peu de temps après. Paul Taylor, neurologue à l'hôpital de recherche pour enfants St.Jude, travaillait à comprendre la génétique des maladies neurodégénératives et a rapporté en 2013 dans Nature que les mutations conservées de HNRNPA2B1 et HNRNPA1 étaient associées à la sclérose latérale amyotrophique (SLA).
En 2015, une renaissance complète était en cours. Cette année-là, cinq articles ont indépendamment démontré que les condensats biomoléculaires étaient cruciaux pour les transitions de phase des condensats biomoléculaires.
Parce que les condensats biomoléculaires sont répandus dans tout le protéome, ces découvertes ont capturé l'imagination des biologistes cellulaires du monde entier.
La recherche sur l'importance des transitions de phase dans la SLA, en particulier, a décollé. Hyman, cofondateur de Dewpoint, a rapporté avec ses collègues que le FUS forme des organites sans membrane sur les sites de dommages à l'ADN et dans le cytoplasme lors du stress, et que les mutations dans le FUS qui sont liées à la SLA conduisent à des transitions de phase aberrantes.
Il semble que les mutations liées à la SLA qui affectent la dynamique de la formation d'organites sans membrane rendent certaines de ces structures plus persistantes qu'elles ne le seraient naturellement. Taylor estime que les perturbations dans les transitions de phase représentent plus de 90% des cas de SLA.
D'autres maladies neurodégénératives pourraient également être liées à la séparation de phase liquide-liquide. En 2017, Ankur Jain et Ron Vale ont proposé qu'un large ensemble de troubles d'expansion répétés - y compris la maladie de Huntington et la dystrophie musculaire ainsi que la SLA - pourraient impliquer la formation de gouttelettes d'ARN aberrantes.
En 2018, Taylor et ses collègues ont rapporté que les espèces de tau solubles, l'un des principaux responsables de la maladie d'Alzheimer, peuvent former des condensats.
Le cancer semble également impliquer la biologie des organites sans membrane.
«La biologie des condensats est le genre de science qui réécrira les manuels - et, selon nous, réécrira la médecine», a déclaré Cary Pfeffer, M.D., directeur général par intérim de Faze et associé chez Third Rock Ventures.
Faze Medicines est fondée par des leaders scientifiques renommés dans le domaine des condensats biomoléculaires:
Roy Parker, Ph.D., est un pionnier dans l'étude de la classe de condensats connus sous le nom de granules RNP avec un accent sur les composants ARN et leur rôle dans les maladies neurodégénératives ainsi que dans d'autres maladies.
Mike Rosen, Ph.D., est un expert de premier plan dans la formation, la régulation et les fonctions des condensats biomoléculaires en mettant l'accent sur les interactions multivalentes qui sont essentielles à leur formation.
J. Paul Taylor, M.D., Ph.D., est un pionnier dans le domaine des transitions de phase liquide-liquide qui a fait des découvertes fondamentales définissant comment les mutations qui modifient ces transitions de phase impactent les maladies neurodégénératives.
Ron Vale, Ph.D., est un expert de premier plan dans les protéines motrices moléculaires qui a récemment démontré comment les ARN d'expansion répétée peuvent entraîner la formation de condensats pathogènes.
D'autres sociétés étudient attentivement les condensats biomoléculaires.
Il y a peu, Nereid Therapeutics avait été lancé avec un financement de 50 millions de dollars, et Transition Bio avait fait ses débuts avec un financement de démarrage non divulgué. Dewpoint Therapeutics, précurseur des condensats, a signé des accords avec deux grands partenaires pharmaceutiques depuis son lancement en 2019. Dewpoint et Nereid travaillent également sur les conditions neurodégénératives, ainsi que sur les applications du cancer.
Faze Medicines se concentre sur les applications dans les maladies neurodégénératives, mais n'a pas encore divulgué de cibles médicamenteuses spécifiques.
À court terme, toutes ces entreprises espèrent inverser la biologie nocive des condensats. Au fur et à mesure qu'elles apprennent à contrôler la composition et le comportement des condensats, ces entreprises pourraient également s'attaquer à des cibles inédites.
Par exemple plutôt que d'inhiber directement une certaine molécule néfaste, un médicament pourrait l'enfermer dans un condensat.
Les condensats nous permettent de penser la découverte de médicaments d'une manière différente.
Les plus grandes firmes pharmaceutiques gardent un oeil sur cette évolution. Dewpoint s'est déjà associé à Bayer sur les maladies cardiovasculaires et gynécologiques et à Merck & Co. sur le VIH.
Faze Medicines prévoit également de s'associer à de grandes entreprises, déclare Cary Pfeffer, PDG par intérim de la société et associé chez Third Rock Ventures.
Novartis Venture Fund, Eli Lilly and Company et AbbVie Ventures ont tous rejoint le syndicat de financement, souligne-t-il, soulignant l'intérêt des grandes sociétés pharmaceutiques pour les condensats.

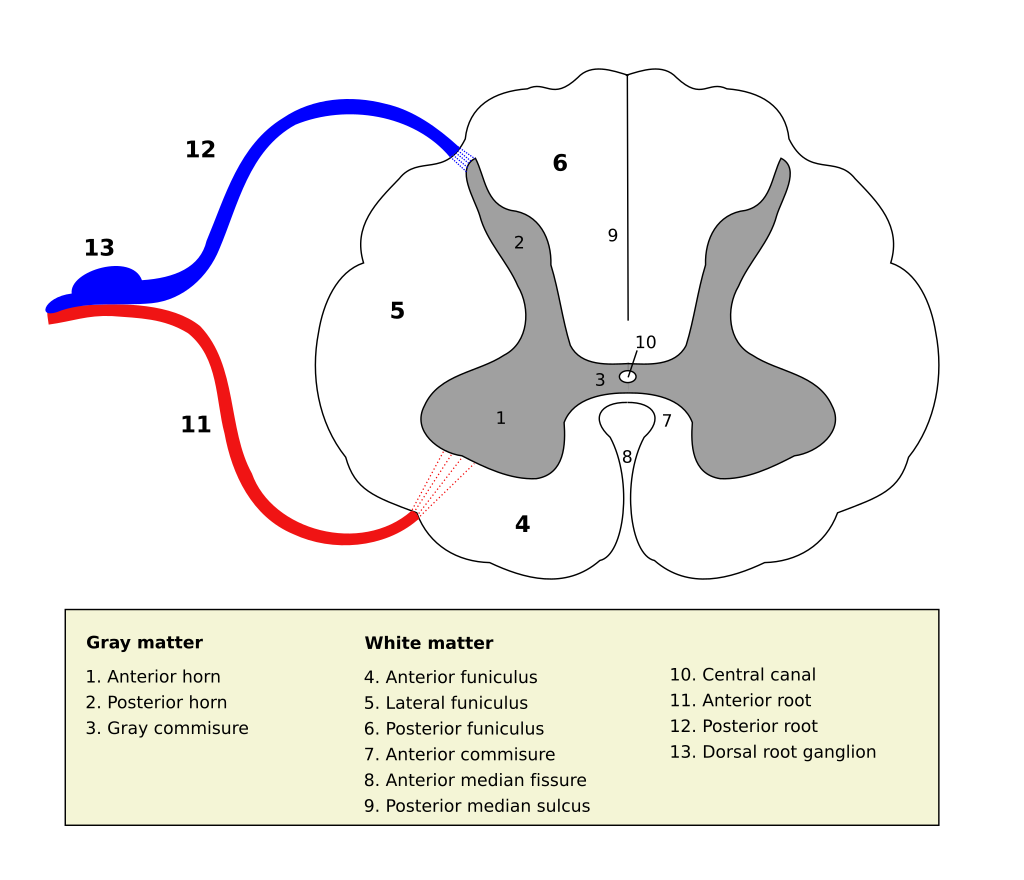 Source Wikipedia/User Polarlys
Source Wikipedia/User Polarlys