Depuis longtemps des patients disent que des régimes alimentaires peuvent soulager des symptomes pour des maladies telles que Alzheimer ou Parkinson. Nombre de malade de la SLA prennent des suppléments en quantité et genre très variés. Ces affirmations ont longtemps été moquées par les scientifiques, pourtant ceux-ci commencent maintenant à changer de point de vue.
Les auteurs d'un nouvel article scientifique ont donc étudié si un régime riche en fibres influence la fonction microgliale chez des souris modèles de la maladie de Parkinson qui surexpriment l'α-synucléine. Ces souris sont appelée souris ASO (α-synuclein overexpressing).
La maladie de Parkinson est une maladie éventuellement caractérisée par une pathologie de l'α-synucléine et/ou un déficit en dopamine résultant de la dégénérescence de la substantia nigra (une région du mésencéphale).
Bien que la maladie de Parkinson soit principalement classée comme un trouble cérébral, 70 à 80 % des patients présentent des symaladie de Parkinsontômes gastro-intestinaux, principalement de la constipation, mais également des douleurs abdominales et une augmentation de la perméabilité intestinale qui se manifestent généralement dans les stades prodromiques (Forsyth et al. 2011 ; Yang et al 2019).
Braak a postulé il y a près de 20 ans que l'agrégation l'α-synucléine peut commencer dans le tractus gastro-intestinal ou le bulbe olfactif, et finalement atteindre le tronc cérébral, la substantia nigra et le néocortex via le nerf vague (Braak et al. 2003). De plus en plus d'éléments corroborent le potentiel de propagation de l'intestin au cerveau de la pathologie l'α-synucléine chez rongeurs (S. Kim et al. 2019 ; B. Liu et al. 2017 ; Svensson et al. 2015).
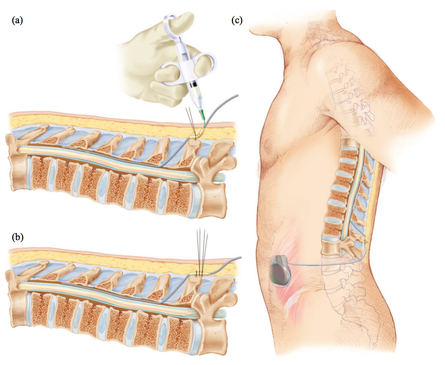
Le nerf vague, un long nerf sinueux, est une voie majeure de signalisation d'informations bidirectionnelles entre l'intestin et le cerveau. La vagotomie est la section chirurgicale du nerf pneumogastrique, ou nerf vague, au niveau de l'abdomen. La vagotomie été utilisée pendant des décennies et la plupart des patients qui ont subi une telle chirurgie et qui sont encore en vie sont maintenant des personnes âgées. Une étude de registre suédoise a étudié le risque de maladie de Parkinson chez les patients ayant subi une vagotomie et a émis l'hypothèse que la vagotomie tronculaire est associée à un effet protecteur.
Les scientifiques ont constaté que le risque de maladie de Parkinson était en effet diminué chez les patients ayant subi une vagotomie tronculaire complète, alors qu'il n'y avait pas de réduction du risque chez ceux qui avaient subi une vagotomie sélective. Le risque de maladie de Parkinson est également diminué après une vagotomie tronculaire par rapport à la population générale. Ces résultats épidémiologiques sont importants et soutiennent l'hypothèse selon laquelle la maladie de Parkinson commence dans l'intestin et non initialement dans le cerveau. Cela fournit une preuve supplémentaire de l'implication du nerf vague dans le développement de la maladie.
De nombreux composants chimiques (de nos jours, nous disons "moléculaires" pour que cela sonne important) importants sont produits dans l'intestin et se retrouvent dans le cerveau via la circulation sanguine. Beaucoup d'entre eux sont fabriqués ou ont leur production régulée par des microbes intestinaux.
Ceux-ci comprennent les acides gras à chaîne courte, le tryptophane, la leptine et la ghréline. Les acides gras à chaîne courte comprennent le butyrate, le propionate et l'acétate. Le butyrate est un inhibiteur connu des histone désacétylases (HDAC) et, ce faisant, agit comme un régulateur épigénétique. Les cytokines, molécules clés de régulation immunitaire produites au niveau de l'intestin, peuvent voyager via la circulation sanguine et influencer la fonction cérébrale, en particulier dans les régions du cerveau où la barrière hémato-encéphalique est déficiente.
Entre autres effets, les métabolites microbiens alimentaires peuvent moduler l'activation de la microglie, or ces cellules nerveuses qui sont indispensables à la survie des neurones sont impliquées dans la maladie de Parkinson. La microglie répond aux signaux provenant de l'intérieur du cerveau, mais reçoit également des informations de la périphérie, y compris du microbiome intestinal (Abdel88 Haq et al. 2019). La microglie de souris adultes exemptes de germes présente un profil d'expression génique immature et ne répond pas adéquatement aux immunostimulants (Erny et al. 2015 ; Thion et al. 2018). Cependant, si l'on nourrit ces souris exemptes de germes avec un mélange d'acides gras à chaîne courte, la maturation microgliale est restaurée (Erny et al. 2015).
Le microbiote intestinal est un organe virtuel qui produit une myriade de molécules dont le cerveau et d'autres organes ont besoin. Les humains et les microbes sont dans une relation symbiotique, les humains nourrissent les microbes, et à leur tour, les microbes fournissent des molécules essentielles aux humains.
Les phylums Bacteroidetes et Firmicutes représentent environ 80 % du microbiote intestinal humain total. Les genres du phylum Firmicutes comprennent Clostridium, Lactobacillus, Bacillus, Clostridium, Enterococcus et Ruminicoccus. Le phylum Bacteroidetes comprend principalement les genres Bacteroides et Prevotella. Le phylum Actinobacterium est dominé par le genre Bifidobacterium. Les bifidobactéries et les lactobacilles sont généralement considérés comme des bactéries bénéfiques et sont fréquemment vendus comme suppléments probiotiques. Des souches du genre Clostridium ou des taxons de lipopolysaccharides tels que les Enterobacteriaceae ont été associées à des états pathologiques dans beaucoup de maladies neurodégénératives y compris la SLA (maladie de Charcot).
Bien que ce soit quelque peu controversé, de façon siilaire le ratio Firmicutes/Bacteroidetes, qui explore la relation entre les deux phylums dominants, a été associé à diverses pathologies neurodégénératives.
Or le microbiome intestinal est altéré dans la maladie de Parkinson. On constate chez les souris modèles de la maladie de Parkinson (on a par génie génétique infligé à ces souris une maladie ressemblant à celle de Parkinson) que les niveaux fécaux des acides gras à chaîne courte sont différent chez les souris malades de Parkinson et les souris saines. Or ce sont les bactéries intestinales qui transforment par fermentation les fibres alimentaires en acides gras à chaîne courte.
Les auteurs ont donc conçus des régimes personnalisés riches en fibres, chacun contenant 20 % d'un mélange prébiotique de deux ou trois fibres alimentaires conçu pour favoriser la croissance de 5 taxons bactériens intestinaux distincts et stimuler la production d'acides gras à chaîne courte sur la base d'une fermentation fécale in vitro.
Les chercheurs ont alors observé de vastes changements au niveau du phylum microbien et du genre après l'administration d'un régime prébiotique, affichant une augmentation des Bacteroidetes et une diminution des Firmicutes chez les souris nourries avec un régime prébiotique, entraînant une baisse du rapport Firmicutes/Bacteroidetes (F/B) qui a été associé à des caractéristiques générales de la santé métabolique.
Curieusement, il a été démontré que les Bacteroidetes sont réduits chez les patients parkinsoniens par rapport aux témoins du même âge, ce qui suggère que le prébiotique peut contrer cet effet (Unger et al. 2016). De plus, ils ont observé une diminution des protéobactéries, un phylum souvent augmenté dans la dysbiose et l'inflammation et élevé dans les échantillons fécaux de patients atteints de maladie de Parkinson (Keshavarzian et al. 2015 ; Shin, Whon et Bae 2015).
Un régime prébiotique riche en fibres atténue les déficits moteurs et réduit l'agrégation de l'α-synucléine dans la substantia nigra des souris.
Parallèlement, le microbiome intestinal des souris ASO adopte un profil corrélé à la santé lors du traitement prébiotique, ce qui réduit également l'activation microgliale.
L'analyse ARN-seq unicellulaire de la microglie de la substantia nigra et du striatum révèle une signalisation pro-inflammatoire accrue et des réponses homéostatiques réduites chez les souris ASO par rapport à leurs homologues de type sauvage suivant un régime standard. L'alimentation prébiotique inverse les états microgliaux pathogènes chez les souris ASO et favorise l'expansion des sous-ensembles de macrophages protecteurs associés à la maladie (DAM) de la microglie.
La microglie dépend de la signalisation du récepteur du facteur 1 stimulant les colonies (CSF1R) pour le développement, le maintien et la prolifération (Elmore et al. 2014).
Pour tester l'effet inverse: Si l'épuisement de la microglie à élimine les effets bénéfiques des prébiotiques, les auteurs ont ajouté PLX5622 au régime alimentaire de souris âgées de 5 à 22 semaines et quantifié le nombre de microglies IBA1+ dans diverses régions du cerveau. PLX5622 est un inhibiteur pénétrant dans le cerveau du CSF1R qui peut épuiser la microglie sans effets observés sur le comportement ou la cognition (Elmore et al. 2014).
L'épuisement de la microglie à l'aide d'un inhibiteur de CSF1R a effectivement éliminé les effets bénéfiques des prébiotiques et rétablit les déficits moteurs des souris ASO malgré un régime prébiotique.
Ces études révèlent une nouvelle interaction dépendante de la microglie entre l'alimentation et les symaladie de Parkinsontômes moteurs chez la souris, des découvertes qui pourraient avoir des imaladie de Parkinsonlications pour la neuroinflammation et la maladie de Parkinson.
Les prébiotiques présentent une approche thérapeutique potentiellement prometteuse, car le régime alimentaire contribue de manière significative à la composition du microbiome et des éléments épidémiologiques ont établi un lien entre les régimes riches en fibres et le risque réduit de développer la maladie de Parkinson (Boulos et al. 2019). Alors qu'une consommation accrue de légumes et l'adhésion à un régime méditerranéen sont associées à un risque plus faible de maladie de Parkinson, les personnes consommant un régime occidental pauvre en fibres et hautement transformé présentent un risque accru de diagnostic de maladie de Parkinson (Alcalay et al. 2012 ; Gao et al. 2007 ; Molsberry et al. 2020). Plusieurs essais cliniques en cours explorent les effets bénéfiques des probiotiques et des prébiotiques sur les résultats liés à la maladie de Parkinson. Agir sur le régime alimentaire ou le microbiome, peut aider à soulager les symptômes de la maladie de Parkinson.

 The imaging analyzes that this study will produce, will make it possible to define a subgroup of patients with Parkinson's disease who will have benefited from the treatment and will help to define rules about when using this therapy in order to avoid unnecessary interventions.
The imaging analyzes that this study will produce, will make it possible to define a subgroup of patients with Parkinson's disease who will have benefited from the treatment and will help to define rules about when using this therapy in order to avoid unnecessary interventions. Deep brain stimulation (DBS) is a neurosurgical procedure involving the placement of a medical device called a neurostimulator, which sends electrical impulses, via implanted electrodes, to specific targets in the brain (the cerebral nucleus) for treatment movement disorders, including Parkinson's disease. illness, essential tremor, dystonia, and other conditions such as obsessive-compulsive disorder (OCD) and epilepsy. Its underlying principles and mechanisms are not fully understood.
Deep brain stimulation (DBS) is a neurosurgical procedure involving the placement of a medical device called a neurostimulator, which sends electrical impulses, via implanted electrodes, to specific targets in the brain (the cerebral nucleus) for treatment movement disorders, including Parkinson's disease. illness, essential tremor, dystonia, and other conditions such as obsessive-compulsive disorder (OCD) and epilepsy. Its underlying principles and mechanisms are not fully understood. In this article, the authors outline the principles of drug selection for Parkinson disease prevention trials, focused on proof-of-concept opportunities that will help establish a methodological foundation for this fledgling field.
In this article, the authors outline the principles of drug selection for Parkinson disease prevention trials, focused on proof-of-concept opportunities that will help establish a methodological foundation for this fledgling field.