Nous sommes dans une période creuse de résultats scientifiques qui durera sans doute tout l'été, aussi voici un résumé d'un article passionnant racontant comment un médecin et chercheur Turque, Sibel Özekmekçi, a développé la maladie de Parkinson, et comment elle a géré cette maladie.
L'article qui est consultable à cette adresse a été résumé, traduit et simplifié pour les besoins du format de publication sur PadiracInnovation.
En tant que neurologue expérimenté spécialisé dans la maladie de Parkinson (MP) et d’autres troubles du mouvement, l'auteur raconte comment elle a diagnostiqué sa propre maladie de Parkinson, qui a commencé par des symptômes très légers.
Dans cet article, elle a choisi de documenter ses observations et ses expériences au cours de ce voyage, en fournissant des informations du point de vue à la fois du patient et du spécialiste.
À travers cet article de synthèse, son objectif était de fournir un compte rendu concis de son parcours scolaire, de son implication professionnelle dans le domaine de la maladie de Parkinson, des premiers symptômes et de la progression de la maladie, des symptômes moteurs et non moteurs associés à la maladie de Parkinson, ainsi que l'impact psychologique de la maladie lors des étapes de reconnaissance, d'acceptation et d'intériorisation.
Après ses études de médecine à la Faculté de médecine d'Istanbul, Sibel Özekmekçi est devenu professeur agrégé et, avec le médecin spécialiste Güneş Kiziltan, ils ont créé le « Groupe de la maladie de Parkinson et des troubles du mouvement » et ont commencé à consulter des patients dans une clinique externe privée.
Dans les années suivantes, ils ont collaboré avec des neurologues et des physiothérapeutes de la Faculté de médecine d'Istanbul de l'Université d'Istanbul pour transmettre les connaissances médicales actuelles sur la maladie de Parkinson aux patients et aux membres de leur famille.
Ainsi l'auteur a souvent soigné des patients atteints de la maladie de Parkinson et occasionnellement des patients souffrant de troubles du mouvement.
A partir de l'âge de 70 ans des contractions involontaires peu nombreuses sont apparus dans le pouce de sa main droite, et même si elle soupçonnait que certaines d'entre elles pourraient signifier un début de maladie de Parkinson, elle a hésité à se diagnostiquer, car les contractions étaient sporadiques.
Elle ne s'y était pas attardée à l'époque, mais en regardant ses photographies prises à cette époque, après le diagnostic, maintenant elle distingue bien la présence d'une légère chute des lèvres du coté droite, ce qui est fréquent chez les patients présentant une maladie de Parkinson.
Puis au fil des ans, des douleurs sont apparues dans la région fémorale antérieure de sa jambe droite lors de longues marches. Elle a aussi fait une chute bénigne en bord de mer, mais sans comprendre la raison de cette chute.
C'est aussi à cette époque qu'elle a remarqué qu'elle se penchait beaucoup en avant lorsqu'elle se promenait et que sa légère bosse, qui était là depuis l'enfance, avait augmenté de taille.
Un jour, alors qu'elle a commencé à avoir des tremblements constants au repos dans le pouce de sa main droite, elle a alors réalisé que le problème était grave.
Le tremblement se présentait sous la forme d'une flexion et d'une extension du doigt, mais elle ne voulait pas encore accepter le diagnostic
Quelques jours plus tard, elle a également eu un tremblement au repos dans l'index de la main gauche, mais cela ne s'est pas reproduit.
De nombreux patients ne consultent pas un médecin à ce stade mais seulement lorsque la maladie progresse et que les symptômes s'accentuent.
Elle a alors consulté un collègue spécialiste de cette maladie.
Aux premiers stades, avant l'âge d'environ 60 à 65 ans, des agonistes dopaminergiques sont prescrits tels que le piribédil en deux à trois doses quotidiennes, le pramipexole à action prolongée en dose unique ou des inhibiteurs de la monoamino oxydase-B tels que la rasagiline en dose unique sont recommandés.
Chez les personnes âgées et chez les patients de tout âge à un stade avancé de la maladie, la lévodopa, est le médicament le plus couramment administré.
Bien qu'âgée alors de 72 ans, elle a cependant préféré se faire prescrire les médicaments adjuvants en raison de la nature légère de ses symptômes et de leur facilité d'utilisation.
Elle n’a pu expliquer le diagnostic à sa fille qu’une vingtaine de jours plus tard, "pour ne pas la bousculer".
Sa fille a été très surprise et, bien sûr, très bouleversée par l'ironie du destin, car Sibel Özekmekçi était médecin et exerçait depuis de nombreuses années dans ce domaine.
Au cours de sa dernière année et demie d'exercice professionel, elle n'a jamais parlé de sa maladie à ses collègues.
À cette époque, elle a également partagé le diagnostic avec son cher ami psychiatre, le Prof. Şahika Yüksel.
Son psychiatre, l'a encouragé à s'ouvrir à ses proches de son état.
Ainsi, un an et demi après le diagnostic, elle a commencé à révéler occasionnellement qu'elle était atteinte de la maladie de Parkinson.
En effet, en partageant le diagnostic avec d’autres, elle avait l’impression que son fardeau s'allégeait.
Elle a alors compris qu’il valait mieux accepter l’apparition des symptômes moteurs.
C'était aussi une relative consolation pour elle de savoir que sa maladie ne faisait pas partie des syndromes « Parkinson plus » dont l'évolution rapide rend les patients handicapés en peu de temps.
Les quelques amis qui connaissaient sa maladie et sa fille lui ont conseillé de faire un suivi auprès d'un autre médecin expérimenté.
Celui-ci a légèrement augmenté la dose de lévodopa/bensérazide.
Pour l'hypersalivation, il a suggéré un collyre au maléate de timolol appliqué sur la langue, qui peut être efficace chez la plupart des patients, mais malheureusement, cela n'a eu aucun effet sur elle.
Cependant, des contractions involontaires des fléchisseurs semblables à une dystonie ont commencé au niveau des deuxième et troisième orteils de son pied droit, particulièrement persistantes l'après-midi et le soir.
Elle a considéré ces contractions comme une dyskinésie induite par la lévodopa, et elle a commencé à prendre un comprimé d'amantadine.
On sait que les patients atteints de la maladie de Parkinson peuvent présenter de nombreux symptômes non moteurs en plus des symptômes moteurs.
Cependant, sans symptômes moteurs, le diagnostic clinique de la maladie est peu probable chez les patients présentant uniquement ces problèmes.
Après confirmation du diagnostic elle a pensé que son insomnie, qui durait depuis 20 ans, pourrait être une manifestation présymptomatique et non motrice de la maladie.
Les symptômes qu'elle a personnellement remarqués chez elle, mais qu'elle a seulement reconnu qu'il s'agissait de signes non moteurs de la maladie après avoir posé le diagnostic sont les suivants :
- Un sentiment de froid
- Beaucoup d’anxiété et de stress extrême.
- Elle a du mal à expliquer ses efforts pour cacher le diagnostic à l'époque ; peut-être ne voulais-elle pas susciter la pitié ou attirer l'attention des autres.
Aujourd'hui, sa maladie est bien contrôlée grâce aux médicaments à la dopamine.
Bien qu’il n’existe actuellement aucun médicament permettant de ralentir la progression de la maladie de Parkinson, il existe des médicaments qui procurent un soulagement symptomatique.
Cependant, même si elle est d’accord avec les récentes observations scientifiques qui montrent que l’exercice ralentit la progression de la maladie, elle doit admettre qu'elle néglige d’en faire régulièrement.
Aujourd’hui, parfois, surtout lorsque elle tient un objet lourd, elle éprouve un léger tremblement dans les deux mains.
Elle a du mal à se relever après être resté assise longtemps, alors elle préfère se lever souvent et marcher pour surmonter ce problème.
En se qui concerne son futur Sibel Özekmekçi sait que dans la maladie de Parkinson, la diminution partielle de la sérotonine et de la noradrénaline dans le cerveau peut conduire à l’émergence d’une dépression chez de nombreux patients. Il a aussi été souligné la présence de diabète de type II chez les patients atteints pourrait constituer un facteur de risque « prodromique » dans le développement de la maladie.
De même, il a été constaté que l'hypothyroïdie et l'utilisation à long terme de lévothyroxine pouvaient également constituer un risque, et la prévalence de cette maladie s'est avérée élevée chez les patients souffrant d'hyperthyroïdie ainsi que hypothyroïdie.
L'auteur doit constamment suivre ses heures de prise de médicaments au cours de la journée et organiser sa vie quotidienne en fonction des intervalles pendant lesquels elle peux manger.
 Indeed, Parkinson’s disease is characterized by the loss of dopaminergic neurons in the substantia nigra pars compacta and the presence of Lewy bodies and Lewy neurites, which mainly consist of aggregates of α-synuclein. It is believed that α-synuclein aggregates poison the brain's cells and indeed especially this tiny part of the brain named "substantia nigra". Yet like other protein aggregates, they may form to protect the brain against some external aggression or stressing event. So the biological mechanisms underlying α-synuclein relationships with dopaminergic neurons have never been firmly established.
Indeed, Parkinson’s disease is characterized by the loss of dopaminergic neurons in the substantia nigra pars compacta and the presence of Lewy bodies and Lewy neurites, which mainly consist of aggregates of α-synuclein. It is believed that α-synuclein aggregates poison the brain's cells and indeed especially this tiny part of the brain named "substantia nigra". Yet like other protein aggregates, they may form to protect the brain against some external aggression or stressing event. So the biological mechanisms underlying α-synuclein relationships with dopaminergic neurons have never been firmly established.
 The hexosamine pathway produces N-linked glycans, essential molecules that support protein folding in the endoplasmic reticulum.
The hexosamine pathway produces N-linked glycans, essential molecules that support protein folding in the endoplasmic reticulum. This initiative may be driven by the pharmaceutical industry's frustration over unsuccessful clinical trials. By using molecular criteria, clinical trials could achieve higher success rates, despite the persistence of clinical symptoms. This strategy is already evident in the Alzheimer's field, where several drugs have been approved without significantly alleviating symptoms.
This initiative may be driven by the pharmaceutical industry's frustration over unsuccessful clinical trials. By using molecular criteria, clinical trials could achieve higher success rates, despite the persistence of clinical symptoms. This strategy is already evident in the Alzheimer's field, where several drugs have been approved without significantly alleviating symptoms. These naked mice allow easy experiments on the skin, application of topical agents, and exposure to UV. To investigate the effects of UV irradiation on hippocampal memory and neurogenesis, mouse skin was irradiated with UV for 6 weeks. After 6 weeks of UV irradiation, the mice underwent behavioral tests. Photoaged mice exhibit impaired cognitive function and neurogenesis.
These naked mice allow easy experiments on the skin, application of topical agents, and exposure to UV. To investigate the effects of UV irradiation on hippocampal memory and neurogenesis, mouse skin was irradiated with UV for 6 weeks. After 6 weeks of UV irradiation, the mice underwent behavioral tests. Photoaged mice exhibit impaired cognitive function and neurogenesis.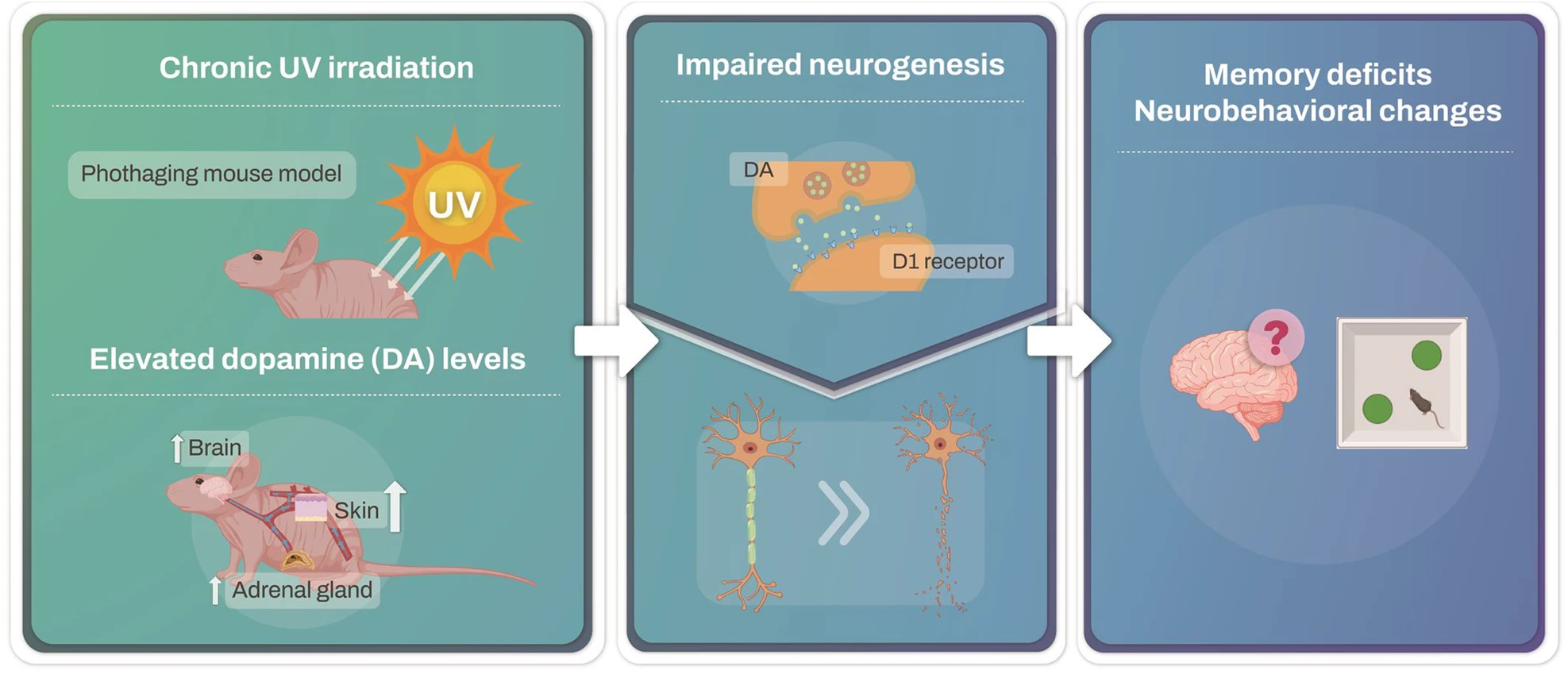 In response to UV exposure, no significant changes in dopamine levels were detected in the ventral tegmental area (VTA), substantia nigra (SN), or hippocampus (HPC). However, dopamine levels in the prefrontal cortex (PFC) and hypothalamus (HT) significantly increased.
In response to UV exposure, no significant changes in dopamine levels were detected in the ventral tegmental area (VTA), substantia nigra (SN), or hippocampus (HPC). However, dopamine levels in the prefrontal cortex (PFC) and hypothalamus (HT) significantly increased. Bien qu'il y est eu de nombreuses études sur la sujet, des
Bien qu'il y est eu de nombreuses études sur la sujet, des